At this point you should have done two consecutive bloodtests. This protocol needs your
most recent Estradiol/E2, Hematocrite/Ht and PSA values for the safety assessement.
2.1 Absolute exclusion criteria
If any of the following absolute criteria are met, do not start TRT:
2.2 Conditional exclusion criteria
If either of these is true, you should start TRT only after these are corrected:
2.3 Informed decision
If both of these are true, go on to step 3
4.1 Measure
- Total Testosterone (tT)
- Estradiol (E2)
- Hematocrit (Ht)
- Free Testosterone (fT)
Measure blood markers right before next injection.
4.2 Overdosing check
If this is true, you MUST decrease the dose:
- Total Testosterone > 31 nmol/L or 900 ng/dL
If this is true, you MUST decrease the dose OR increase the injection frequency:
- Hematocrit (Ht) > 54% or 0.54
If this is true, you MUST decrease the dose OR increase the injection frequency OR lose
bodyfat:
- Estradiol > 220 pmol/L or > 60 pg/mL
4.3 Underdosing check
If either of these is true, you should increase the dose:
If needed adjust dose in small amounts only, e.g. 20% or
20-30mg/week.
4.4 Injection frequency check
If you feel stable (no mood or energy swings related to the injection cycle) you can try
a longer interval, else you can try a shorter interval. Adjust the dose accordingly.
Always work with weekly doses divided by number of injections per week. Higher frequencies
are safer.
5.1 Periodic evaluation
After starting TRT, patients should undergo a focused evaluation at 6 months and then
yearly to ensure safety, efficacy, and timely adjustments. Each assessment involves both
laboratory tests and clinical examinations, with results interpreted using both EU (SI)
and US (conventional) units.
- Total Testosterone (tT)
- Free Testosterone (fT)
- Hematocrit (Ht)
- Prostate-Specific Antigen (PSA)
- Estradiol (E2)
- Liver Function Tests; ALT/AST to detect hepatotoxicity
-
Lipid Profile; Total cholesterol, LDL, HDL, triglycerides—evaluate cardiovascular
risk
- Fasting Glucose or HbA1c; Screen for insulin resistance
- Blood Pressure
-
Clinical Exam; Evaluate mood, libido, energy, sleep quality, injection sites, and
any adverse effects
- Lifestyle Screen
-
Psychological Screen; Assess for depression, anxiety, and quality-of-life metrics
-
Review of Comorbidities: Update on cardiovascular events, prostate
symptoms (IPSS score), sleep apnea status, and fertility desires.
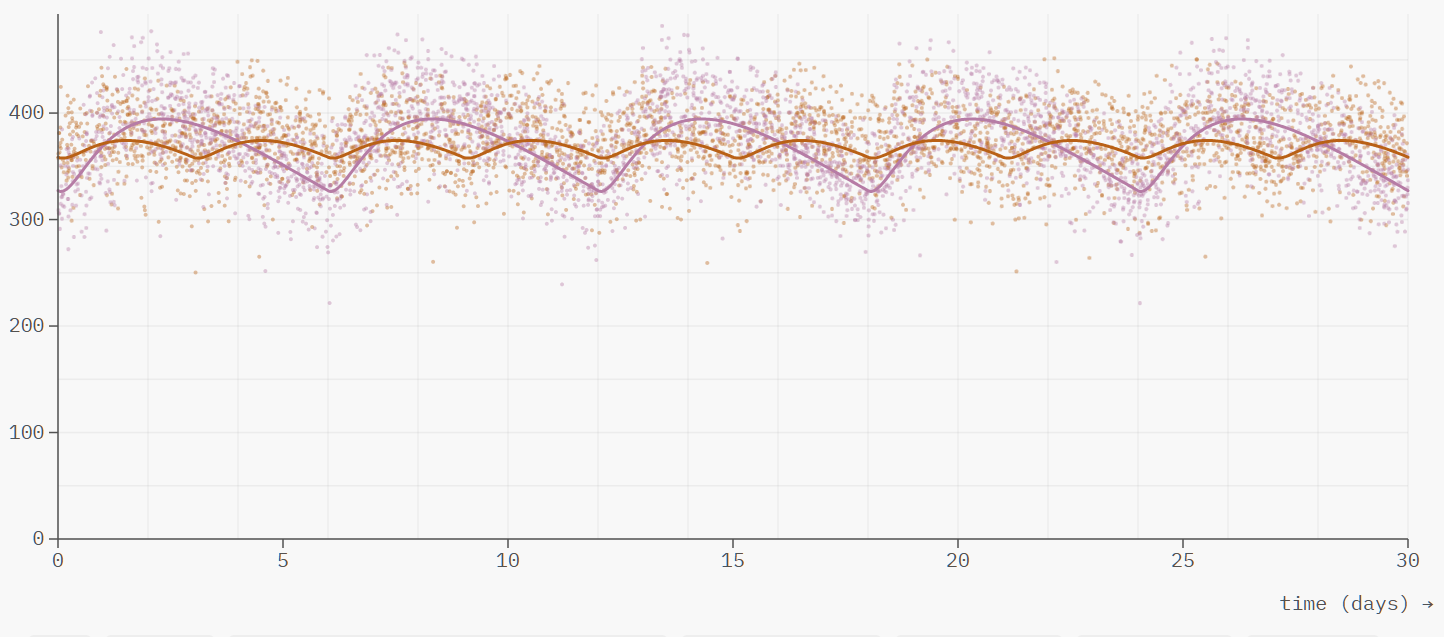 Comparing a 30mg/3days and a 60mg/6days protocol (cypionate)
Comparing a 30mg/3days and a 60mg/6days protocol (cypionate)